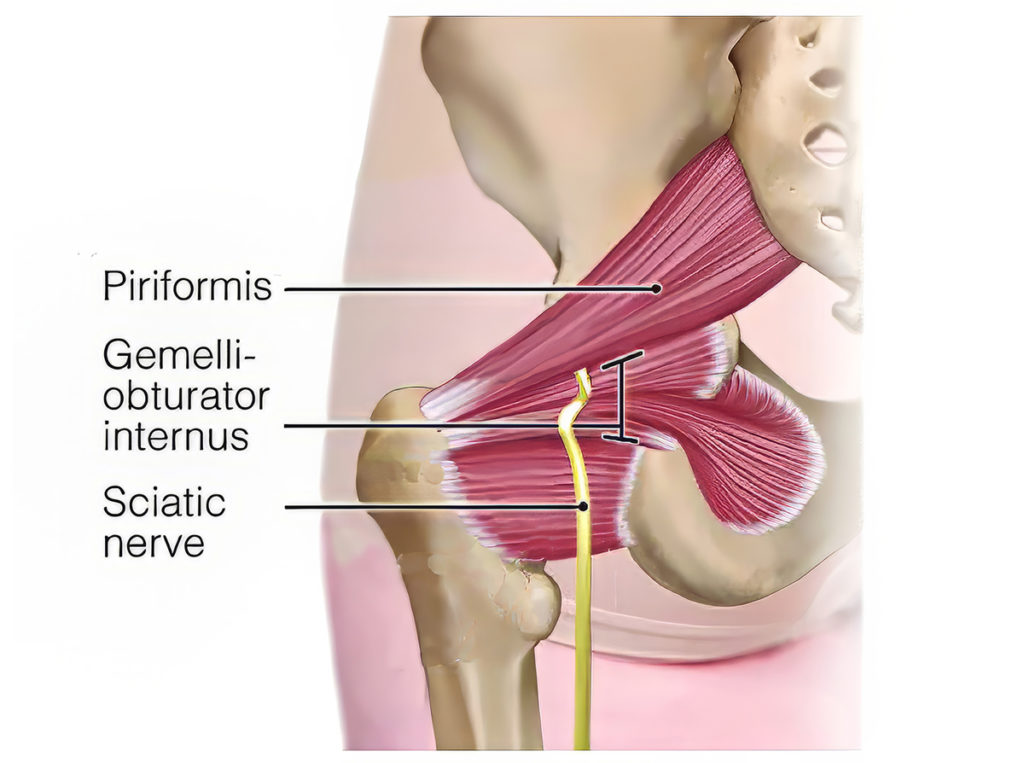
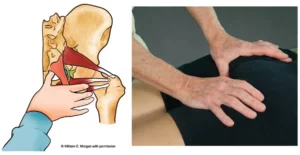
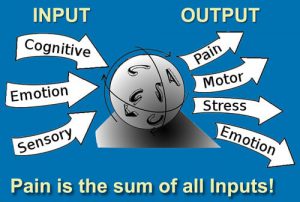
The buttock has been assigned more syndromes than any other bodily region. This is due to the biomechanical complexity of the sciatic nerve and the tremendous torsional forces traversing the pelvis and lumbar spine during daily activities. Piriformis syndrome, gemelli-obturator internus syndrome, ischial tunnel syndrome, and greater trochanteric pain syndrome are but a few of the names used to describe symptoms associated with tendinopathies and sciatic-nerve entrapment sites in the buttocks. Special orthopedic tests may help rule out possible offenders, and a comprehensive intake aids in detecting biopsychosocial factors that may be contributing to the client’s pain. However, the problem I often encounter when assessing buttocks pain is symptom overlap, which can make pinpointing the exact location difficult and unreliable. So, in this blog, I’ll use the umbrella term deep gluteal syndrome (DGS) to describe generalized sciatic-related buttock pain. I’ll also outline a few techniques I’ve found helpful in freeing up musculofascial tissues that may be possible perpetrators.