Q: How can manual therapies be used to help eliminate pain?
Erik Dalton responds:
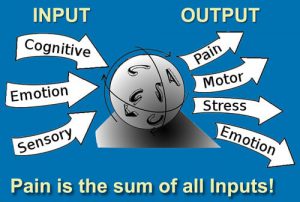
Working in the pain-management field is a challenging, yet exceptionally rewarding, experience. Clients suffering from chronic pain are confronted by a unique disorder—a personal experience unlike any other physical malady. While a broken bone can be confirmed by an X-ray and an infection can be detected by a simple blood test, there are no universally reliable tests available to measure pain levels. Because of this, many common musculoskeletal complaints are incorrectly assessed and treated.
Typically, when a person experiences a slight sacroiliac joint sprain it’s often hard to pinpoint the exact pain site, since everything in the back, hip and leg seems to hurt. It’s often necessary to feel around the whole area to determine the exact site of the pain’s origin. Thus, to localize and identify the pain, it’s usually necessary to draw on central nervous system (CNS) modalities, such as sight, movement response and touch.
Recall what happens when you pinch a worm—it curls towards the pinch. And when holding a newborn baby, try this experiment: Place the baby face down with the stomach resting in your palm, so its back faces you. Allow the baby’s hips to move, with each leg straddling your arm. By running your finger down the back about one inch lateral to the spine, you’ll see the Landau reflex. The baby’s erector spinae muscles will automatically contract on the side where the stimulus is applied. There is very little difference between this reaction and the reaction that occurs when a painful stimulus is applied to the spine later in life: The erector spinae muscles, including the transversospinalis, automatically and involuntarily contract toward the side of injury.
In adults, locked facet joints and strained spinal ligaments are major culprits perpetuating this ingrained reflex. Reflexogenic myospasm from motion-restricted joints results in decreased oxygen supply to surrounding tissues and resultant toxicity, adhesion and fibrosis.
Left untreated, continuous neural bombardment triggers stubborn pain-spasm-pain reflexes that amplify musculoskeletal tone (protective muscle guarding), distort posture (functional scoliosis) and up-regulate sympathetic nervous system activity (anxiety). Regrettably, the brain has the ability to learn these aberrant postural patterns as normal. Neuroscientists label this condition—where distorted postures remain in the body long after the original stimulus has been removed—as spinal learning, reflex entrainment and neuroplasticity.
Deep intrinsic (postural) slow-twitch muscles, such as the iliopsoas, transversus abdominis and semispinalis, burn oxygen for fuel (oxidative metabolism) and are fatigue-resistant when exercised, stretched and maintained properly. We live in a flexion-addicted society where sitting is the norm. Computer addicts, folks who drive for a living and couch potatoes constitute only a small group whose inactivity level causes deep anti-gravity support muscles to neurologically shorten and distort posture.
As the pectorals overpower the lower shoulder stabilizers and the trunk flexors overpower the hip extensors, weight shifts to the fast-twitch extrinsic muscles, which burn glucose for fuel (glycolic metabolism). Since extrinsic muscles aren’t designed to battle gravitational exposure, weight soon shifts back to the oxygen-starved and fatigued intrinsic muscles. Unable to maintain the body’s anti-gravity support system, these overworked postural structures reluctantly dump the compressive load to the spine and pelvis.
This sets the stage for what the medical establishment loosely calls degenerative disc disease. As increased weight-bearing flattens intervertebral discs and crams facet joints together, the posterior longitudinal ligament becomes lax. Forward-bending, twisting or whiplash incidents can tear the ligament away from the bony margins and vertebral end plates, causing internal pressure to fill the cracks with calcium or bone spurs. Osteophytic spurs gradually begin to fill the intervertebral foramina and can impinge on nerve roots or the spinal cord (spinal stenosis).
This common osteoarthritic condition is the number-one cause of long-term neck pain. Fortunately, if discovered in the early stages, systematic mobilization of fibrotic tendons, ligaments and joint capsules often frees the restricted dural membrane and offers some relief. But the condition can return unless whole-body structure, function and balance are properly restored.
Most of our clients battling recurrent pain (including fibromyalgia, chronic fatigue and backache) are trapped in either an intrinsic or extrinsic state of collapse. Too often, we settle for immediate symptom alleviation rather than digging for the root of the problem.
As the great Czech researcher Vladimir Janda, M.D., once said, “The neuromusculoskeletal system must be assessed and treated as a whole, with muscle dysfunction considered in relation to the functional status of the whole motor system, including articular and nerve structures. Any change in the statics or dynamics of the distal trunk and lower extremities will, in some way, be mirrored in the function of the upper complex, and vice-versa.”
Traditional massage of a peripheral pain site temporarily calms cutaneous skin and fascial receptors, thus reducing superficial pain. But to alleviate deep-seated, joint-complex pain, the client must be actively involved.
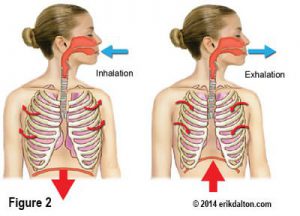
For example, many have acquired a habit of sitting and holding a telephone on one shoulder while performing other tasks. Sustained hypercontraction of the upper trapezius, levator scapula and associated fascia causes cervical and thoracic facet joints to lock closed on the ipsilateral side creating alterations in normal mechanoreceptive input to the brain. To calm the irritated articular receptors and release the accompanying protective muscle guarding, the therapist must hold superiorly-directed sustained pressure to deep transversospinalis muscles (overlying the fixated joint), while the client engages the area with some sort of movement. Chin-tucking is an excellent enhancer for stuck thoracic vertebrae, and pelvic-tilting helps mobilize fixated lumbar vertebrae. The use of enhancers, such as pelvic-tilts for low-back and pelvic pain, deep breathing for diaphragm/scalene releases, limb movements for glenohumeral restrictions and chin-tucking for cervical and upper thoracic restrictions, normalizes afferent activity and helps break stubborn reflexogenic pain-spasm-pain cycles.
To achieve a noticeable reduction of increased excitability in the neuronal pool, the pain-generating stimulus must be interrupted until the memory burned into the nerve cells has been completely forgotten. For many chronic-pain cases, a serial-type deep-tissue therapy works best when clients are seen twice weekly until hyperexcited receptors feeding the CNS are quieted. This will eventually inhibit the chemical activation of pain at the site of its peripheral stimulation.
Of course, successful management of chronic pain depends on much more than intellectual knowledge. It must be teamed with keen observation skills, patience, compassion and a constant reminder that the healer is, ultimately, within each client. Therapists serve only as helpful facilitators in the ongoing journey toward optimum health and they should gratefully utilize the body’s innate self-regulatory system to help guide the therapeutic process.
Despite the variety of pain-management approaches available in today’s ever-expanding bodywork field, the therapeutic goal should remain the same: restoration of maximal pain-free movement within postural balance.
Posted by permission of MASSAGE Magazine. Originally published in MASSAGE Magazine’s Expert Advice column, April 2008.
Click here for more information.
On sale this week only!
Save 25% off the Posture Pain Performance course!
NEW! USB version with enhanced video
Discover the foundational principles behind MAT technique as we take you on an in-depth look at the connection between pain, posture and function. Save 25% off the Posture Pain Performance course this week only. Offer expires Monday April 22nd. Click the button below for more information and to purchase the course. Upon completion receive 20CE hours and a certificate of completion to display in your office.
Bonus: Order the Home Study version and receive the e-Course for FREE!