 A frequently asked question in Myoskeletal Alignment seminars is how to differentiate sacroiliac from piriformis syndrome symptoms. Indeed, these structures are often involved in a symbiotic relationship. Length/strength piriformis imbalance strongly influences movement of the sacrum between the two hip bones and clinically, we know both can cause sciatic-like symptoms… a condition which affects nearly 40 percent of adults at some point during their life.
A frequently asked question in Myoskeletal Alignment seminars is how to differentiate sacroiliac from piriformis syndrome symptoms. Indeed, these structures are often involved in a symbiotic relationship. Length/strength piriformis imbalance strongly influences movement of the sacrum between the two hip bones and clinically, we know both can cause sciatic-like symptoms… a condition which affects nearly 40 percent of adults at some point during their life.
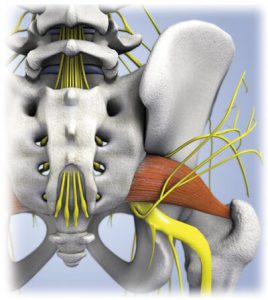
But, unlike sacroiliac joint dysfunction, piriformis pain is classified as a “functional entrapment syndrome” resulting from a positional abnormality in which the sciatic nerve becomes compressed between piriformis and either the sacrospinous ligament and/or, the bony sciatic notch. The word functional describes neurological compression disorders resulting from positional or kinesiological factors that are not solely linked to structural or inflammatory conditions. Therefore, clients presenting with piriformis syndrome typically only experience sciatic-like symptoms during certain movements or when pressure is applied to the affected area.
The burning question is… why are some clients symptomatic and others not?
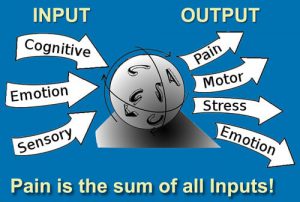
Obviously, the brain’s interpretation of possible nerve damage is the key factor resulting in symptoms such as sciatic pain or protective muscle guarding, but genetics may also play a role. In some clients the sacrospinous ligament is positioned more superiorly in the sciatic notch leading to a greater predisposition for this type of dural entrapment syndrome.
Much like lumbar intervertebral disc herniations, the sciatic nerve must be squashed against something to trigger intraneural edema and accompanying neurological symptoms such as pain, numbness, tingling and weakness. In some cases, sciatic nerve axons may experience a double-crush condition beginning with damage from lumbar discs or osteoarthritic spurs and get compressed again under the piriformis.
In past blogs I’ve discussed lumbar and pelvic mobilization approaches, so in the following technique description and accompanying video, I’ll demo one of my favorite piriformis graded exposure stretches.
Myoskeletal Piriformis Technique

GOAL: Relieve external hip rotator compression
ACTION:
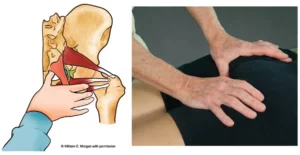
- Therapist places client’s right foot on the lateral side of her opposite knee
- Therapist’s right hand pushes client’s hip into adduction in order to lift the hip off the table allowing his knee to contact client’s lateral hip rotators
- Therapist’s left hand contacts client’s left ASIS
- Therapist gently pulls on client’s knee and uses his knee as a tool to work her tight hip external hip rotator muscles
- Therapist rocks the leg and hip back and forth using his knee as a fulcrum on the hip rotatorsRepeat 3 to 5 times on affected side (pain free)
References
1. McCrory P, Bell S. Nerve entrapment syndromes as a cause of pain in the hip, groin and buttock. Sports Medicine
2. Retzlaff E, Berry AH, Haight AS, et al. “The Piriformis Muscle Syndrome. Journal of the American Osteopathic Association; 73:799-807.

Techniques as presented in The ART of MAT Home-Study Course
On sale this week only!
Save 25% off the "Dalton Technique Treasures" eCourse

The “Dalton Technique Treasures” eLearning course is a compilation of some of Erik’s favorite Myoskeletal Alignment Techniques (MAT). Learn MAT techniques to assess and address specific sports injuries, structural misalignment, nervous system overload, and overuse conditions. ON SALE UNTIL April 29th! Get Lifetime Access: As in all our eLearning courses, you get easy access to the course online and there is no expiry date.