Forward Head Posture
“For every inch of Forward Head Posture, it can increase the weight of the head on the spine by an additional 10 pounds.” -Kapandji, Physiology of Joints, Vol. 3
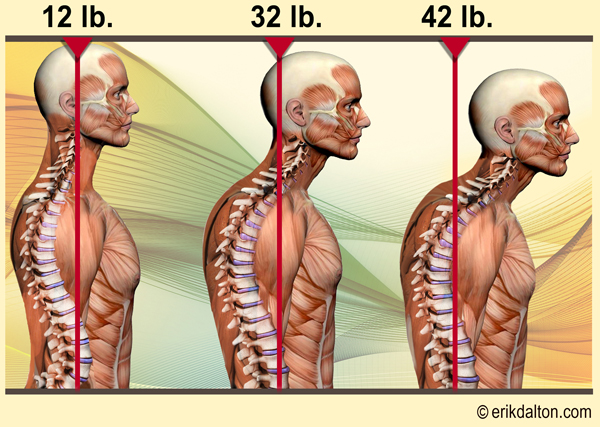
It’s not uncommon to have clients walk into your office sporting a 12 pound head that’s migrated three inches forward of their shoulders. You know prior to palpation that their cervical extensors (semispinalis, splenii, longissimus and upper traps) are in a losing battle attempting to isometrically restrain 42 pounds against the unrelenting force of gravity (Fig. 1).
Rene Cailliet M.D., former director of the department of physical medicine and rehabilitation at the University of Southern California wrote:
- Head in forward posture can add up to thirty pounds of abnormal leverage on the cervical spine. This can pull the entire spine out of alignment.
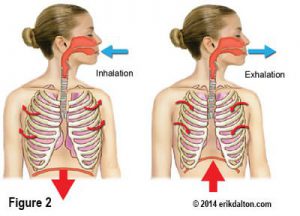
- Forward head posture (FHP) may result in the loss of 30% of vital lung capacity. These breath-related effects are primarily due to the loss of the cervical lordosis which blocks the action of the hyoid muscles, especially the inferior hyoid responsible for helping lift the first rib during inhalation.
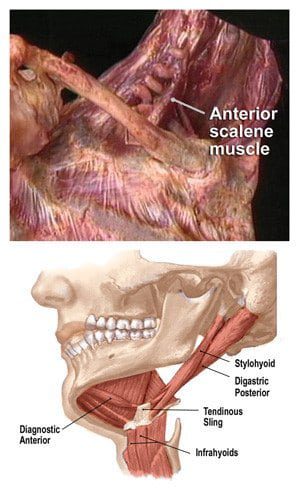
- Proper rib lifting action by the hyoids and anterior scalenes is essential for complete aeration of the lungs(Fig 2: Hyoids/ant scalenes).
- The entire gastrointestinal system (particularly the large intestine) may become agitated from FHP resulting in sluggish bowel peristaltic function and evacuation.
- Cailliet also states: “Most attempts to correct posture are directed toward the spine, shoulders and pelvis. All are IMPORTANT, but, head position takes precedence over all others. The body follows the head. Therefore, the entire body is best aligned by first restoring proper functional alignment to the head”. 1
The effects of poor posture go far beyond just looking awkward.
In fact, the January, 2004 issue of the American Journal of Pain Management reported on the relationship of poor posture and chronic pain conditions including low back pain, neck related headaches, and stress-related illnesses. “The extra pressure imposed on the neck from poor posture flattens the normal cervical curve resulting in abnormal strain on muscles, ligaments, fascia and bones.”2
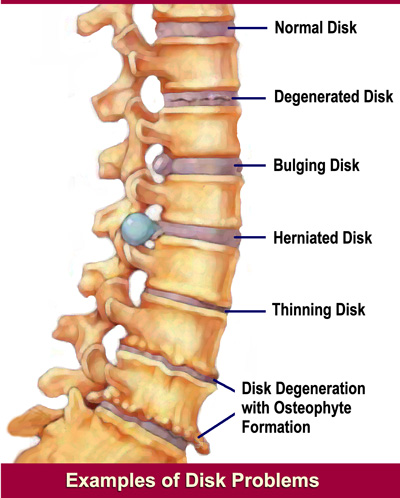
Research presented at the 31st Annual International Conference of the IEEE EMBS Minneapolis, Minnesota, USA, (2009) stated; “Over time poor posture results in pain, muscle aches, tension and headache and can lead to long term complications such as osteoarthritis. Forward head carriage may promote accelerated aging of intervertebral joints resulting in degenerative joint disease.”3 (Fig. 3).
It appears posture impacts and modulates all bodily functions from breathing to hormonal production. Spinal pain, headache, mood, blood pressure, pulse and lung capacity are among the many conditions influenced by faulty posture.
“90% of the stimulation and nutrition to the brain is generated by the movement of the spine” Dr. Roger Sperry, (Nobel Prize Recipient for Brain Research)
Additionally, Dr Roger Sperry demonstrated that 90% of the brain’s energy output is used in relating the physical body to gravity. Only 10% has to do with thinking, metabolism, and healing.4
Consequently, a FHP will cause the brain to rob energy from thinking, metabolism, and immune function to deal with abnormal gravity/posture relationships and processing. The March 2000 Mayo Clinic Health Letter expounded on Sperry’s findings by reporting that prolonged FHP also leads to “myospasm, disc herniations, arthritis and pinched nerves.” Degenerative neck pain goes hand-in-hand with balance problems especially in the elderly. Sensitive cervical spine mechanoreceptors govern the body’s ability to balance and must be perfectly coordinated with the inner ear’s vestibular balance system to stabilize equilibrium in both static posture and gait. Keeping the eyes looking forward is a basic life-preserving reflex, and as such, dominates nearly all other postural considerations. Proprioceptive signals from the first 4 cervical vertebrae are a major source of stimuli for regulating the body’s pain-controlling chemicals (endorphins). FHP dramatically reduces endorphin production by limiting the cervical spine’s range of motion. Inadequate endorphin production up-regulates the central nervous system causing non painful sensations to be experienced as pain. Fig. 4 shows a couple of good mobilization techniques to restore joint-play to upper cervical fixated facets.

Dr. Alf Breig, a Swedish neurosurgeon and Nobel Prize recipient coined the termed ‘adverse neural tension’ to describe the mechanism by which loss of normal cervical lordotic curve creates dysfunction and disease.5
Through cadaver studies, Dr. Breig demonstrated that neck flexion could stretch the spinal cord 5-7 cm causing tensioning of the meninges (covering of the brain and spinal cord) and elicit measurable pressure on brain-stem nuclei (nerve control centers) which control all basic life functions. The increased compression led to dysregulation of basic metabolic control functions. Recall that the spinal cord is actually only “tethered” to the bony skeleton in the upper cervical and lowest sacral areas TOP and bottom ends of the spine). In between these polar attachments, the spinal cord is relatively free to move up and down. Free-floating mobility of the cord is essential in allowing bending and twisting of our bodies. Anything that reduces that freedom, i.e., exaggerated or flattened spinal curves, dural impingement, etc. increases cord and brain stem tension. Increased tensile stress on the cord and brain stem not only interferes with the control of basic body processes such as breathing and motor control but in cases of dural impingement, may encourage painful cervical radiculopathies.
Identifying Common Compensatory Patterns
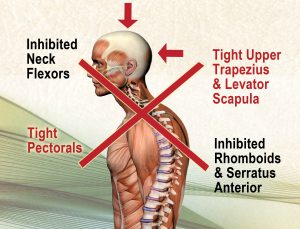
Fortunately, the legendary biomedical researcher Vladimir Janda, MD has helped simplify assessment of commonly seen muscle imbalance patterns consistent with FHP. Janda’s Upper Crossed Syndrome(Fig. 5)is characterized by overactivity or tightness in the upper trapezius, levator, suboccipitals. sternocleidomastoids and pectoralis major and reciprocal weakness of the deep neck flexors and lower scapular stabilizers. Trained therapists visually recognize this aberrant pattern through postural and gait analysis and kinesthetically through tissue palpation and muscle length testing. Unfortunately, as normal movement patterns are altered by persistent pain, joint fixations or muscle imbalances, new neuronal pathways are burned into the central nervous system and gradually memorized as normal (neuroplasticity). Any deviation of normal head and neck movement alters precise firing order patterns causing the prime mover to be slow to activate. Substitution patterns develop as synergistic stabilizing muscles are recruited to do the job of the prime mover. Some believe the first step in restoring proper muscle balance is to mobilize dysfunctional joints to help reprogram these garbled neuromuscular pathways. Once normal joint play is established and muscle splinting removed, structural integrative soft tissue work creates functional length/strength balance.
Correction of Upper Crossed neck posture is key to stopping and possibly reversing decay, degenerative changes and pain from headaches, rib dysfunction, TMJ, and Dowager’s Humps …but it takes time and a concerted effort to repair the damage caused by faulty neck posture.
The following traits are often seen in those presenting with Upper Crossed Syndrome:
- Suboccipital pain syndromes
- Mouth breathing (sleep apnea)
- Difficulty swallowing
- Teeth clenching
- Face & neck pain
- Migraine headaches
- Uncoordinated gait and loss of body balance
Summary
Often seen as a structurally subtle body segment, the neck is burdened with the challenging task of supporting and moving the human head. Because of tension, trauma and poor postural habits inherent in today’s workplace, it comes as no surprise that head-on-neck and neck-on-thorax disorders rank high among the most common pain GENERATORS driving people into bodywork practices. When spinal tissues are exposed to continued compression, they deform and go through a transformation that can become permanent. Correction of Upper Crossed neck posture is key to stopping and reversing degenerative joint disease and pain from headaches, rib dysfunction, TMJ, and Dowager’s Humps. English philosopher Bertrand Russell once stated, “A physical system expresses its energy through function”. Any loss of function sets off reactions within the body’s open, dynamic system which manifests as structural abnormalities…and vice-versa. When treating functional problems such as loss of joint play, therapists must look beyond the symptoms and the artificial dividing of the body into systems and treat the whole.
On sale this week only!
Save 25% off the Posture Pain Performance course!
NEW! USB version with enhanced video
Discover the foundational principles behind MAT technique as we take you on an in-depth look at the connection between pain, posture and function. Save 25% off the Posture Pain Performance course this week only. Offer expires Monday April 22nd. Click the button below for more information and to purchase the course. Upon completion receive 20CE hours and a certificate of completion to display in your office.
Bonus: Order the Home Study version and receive the e-Course for FREE!