Treating the TMJ
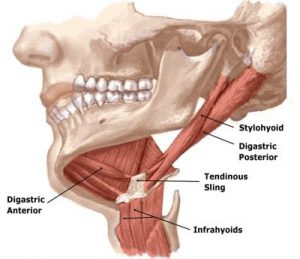
It’s not uncommon to be in the final stages of a history intake when the client casually states, “Oh, there is one other thing — sometimes my jaw clicks when I eat or open my mouth”. A clicking jaw in those presenting with face, head and neck pain may be a smoldering fire that should not be ignored. Joint noise is not unusual, but a clicking jaw can represent an incorrect condyle-disc-mandibular fossa relationship or possibly osteoarthritis (Image 1).

I find it’s best to address jaw-related muscle imbalance patterns before the disc(s) becomes irreversibly deformed. A systematic review by Medlicott and Harris found that active exercise, manual mobilizations and postural training may be effective in treating temporomandibular joint (TMJ) disorders.1 However, many therapists choose not to treat the condition unless the client is experiencing pain. I believe this represents a missed opportunity to address anatomical and functional problems in their early stages.
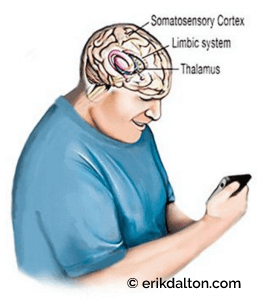
When the head and neck move forward in the sagittal plane, the brain’s visual proprioceptors cause the occiput to backward-bend on atlas. This remarkable brain stem reflex (Law of Righting) will cock the head back to level the eyes against the horizon even if it means ravaging the neck.
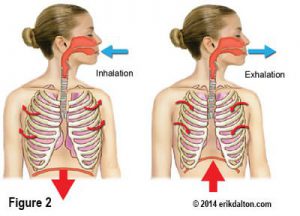
Sustained isometric contraction in the suboccipitals reflexively weakens the longus capitis and colli antagonist muscles and places the entire nervous system in a heightened state of alert. With the head and neck jutted forward, passive tensile forces develop in the hyoid and digastric muscles (Image 2).
The brain, in essence, is trying to compensate for the forward head carriage by pulling back on the cranium using the jaw muscles. Prolonged hypercontraction in these jaw openers stresses the TM joint as the mandible is forced to translate posteriorly and inferiorly…a condition called jaw retrusion.
This may be problematic since the hyoids, digastrics, and the lateral pterygoids are jaw openers and the brain doesn’t like us to walk around with the jaw hung open. So, the only recourse the brain has now is to call on powerful jaw closers such as the temporalis, masseter and medial pterygoid muscles.
Thus, the battle begins and the mouth closers usually win, but at a terrible cost to the TM joint and neck. Antagonistic co-contraction of these muscle groups may promote abnormal mandibular positioning, nerve entrapment, ligamentous strain, and disc compression, leading to the TMJD disorders we commonly see in our massage and bodywork practices.
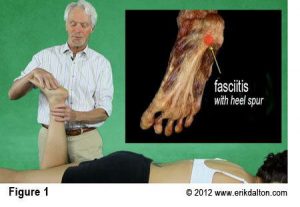
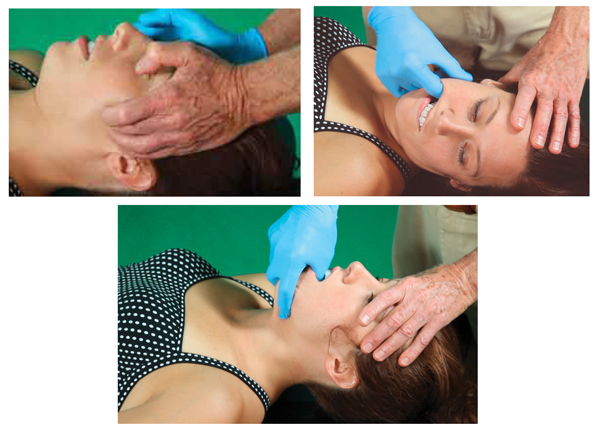
In Myoskeletal Therapy, we begin by creating a level platform at the occipitoatlantal (O-A) joint and then perform a basic TMJ routine such as the one shown in this video. Home retraining exercises such as the “chin-tuck” is suggested to help reinforce the work.
On sale this week only!
Save 25% off the Posture Pain Performance course!
NEW! USB version with enhanced video
Discover the foundational principles behind MAT technique as we take you on an in-depth look at the connection between pain, posture and function. Save 25% off the Posture Pain Performance course this week only. Offer expires Monday April 22nd. Click the button below for more information and to purchase the course. Upon completion receive 20CE hours and a certificate of completion to display in your office.
Bonus: Order the Home Study version and receive the e-Course for FREE!