Myoskeletal Muscle Manipulation Through Joint Mobilization
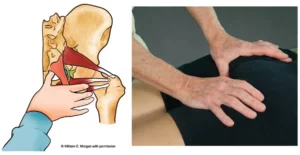
A confounding situation arises as the therapist’s fingers attempt to pry between joint surfaces to contact the short rotators, intertransversarii, and intertransverse muscles. Although these tiny, one-joint rotators/side-benders typically are the tightest in the presence of joint dysfunction, application of direct localized pressure sometimes is impossible, given the limited space between articular surfaces. Here’s when the myoskeletal technique comes in handy. The therapist utilizes sustained manual pressure on the superior fixated vertebra as the joint is taken through a specific range of motion. Basically, bones are used as levers to create a Golgi tendon organ (GTO) release in all fourth-layer muscles, causing the joint blockage. The question then arises as to the NATURE of the fixated joint: Is it locked, open or closed? And which side of the spine is stuck?
Using the myoskeletal approach, the therapist’s fingers and thumbs wade through the paraspinal laminar groove tissues, scanning for lumpy, wiry and knotty transversospinalis muscles. Once the hypertonic little muscles are found, what information is revealed about the nature of the dysfunctional joint? Not much! By Greenman’s definition, it’s obvious that joint dysfunction exists, but what type? Is one side of the joint jammed closed and unable to open during forward bending, or is a superior facet not closing on the vertebra below during backward bending?
Stuck Closed
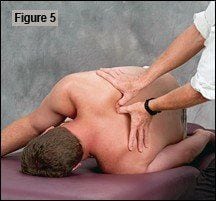
In Figure 5, the therapist’s thumbs apply sustained pressure to the bony knot where the fibrosis was found, as the side-lying client flexes and extends the spine through the affected area using a chin-tucking enhancer. If the bony knot pushes back into the thumbs as flexion is introduced, the joint on the ipsilateral side is not opening. The joint’s axis of rotation is forced to revolve around the fixated facets, causing the superior transverse process to push back against the therapist’s thumbs. The thumbs hold a gentle, sustained headward pressure on the superior transverse process as the client flexes the chin toward his chest. This produces a GTO release in the deep groove muscles and stretches the fibrosed spinal ligaments and joint capsule, allowing the fixated facets to open. In the myoskeletal method, bones are only applied as levers to release adhesive spinal soft tissues that cannot be liberated directly with traditional deep-tissue techniques.
During the fourth-layer assessment, if the bony knot does not push back into the palpating thumbs or fingers as the client flexes through the area, the joint is not closing on the contralateral side. To free the hypertonic tissues preventing closure of the superior facets on their inferior neighbor, the client assumes a prone position. The therapist’s fingers, thumbs or elbow slowly glide down each side of the lamina groove as the client rhythmically raises and lowers his head. In Figure 6, the therapist uses the elbow to traverse down the groove while the client extends and lowers his neck and upper thoracic spine. If a bony knot is palpated, the joint is not closing on the contralateral side. Gentle, sustained pressure (with client-enhancing movement) releases fibrotic groove muscles, joint capsules, and spinal ligaments, allowing the superior facets joints to glide inferiorly and close on the vertebra below.
Scope of Practice
As with all treatment protocols, exceptions occur that can render the myoskeletal method ineffective. Damaged joints often create stubborn fixations that cannot be released by working muscles alone. Vertebrae that have undergone adherent cartilage degradation, apophyseal joint swelling and facet “nipping” due to prolonged microtrauma, typically will not regain lost motion simply by releasing the fibrotic muscles, joint capsules and spinal ligaments. True adhesive joint-fixation problems point to a more serious condition. However, massage therapists who regularly work in conjunction with chiropractors and manipulative osteopaths can enhance therapeutic outcomes by “prepping” the affected area, so that high-velocity thrusting maneuvers are more effective. Manual therapists must develop a good complementary health care referral base so prompt referrals can occur if soft-tissue approaches do not alleviate all the client’s pain and/or posture problems.
Combining muscle and joint modalities increases therapeutic efficiency and encourages referrals as therapists resolve stubborn, long-standing pain/spasm/pain CYCLES. By incorporating holistic-minded reflexogenic routines, today’s touch therapist can help solve America’s epidemic musculoskeletal pain crisis. Therapeutic outcomes are enhanced as assessment and treatment routines are expanded to include all soft tissues forming from the mesoderm, including muscles, fascia, joint capsules, spinal ligaments, nerve dura, and intervertebral discs.
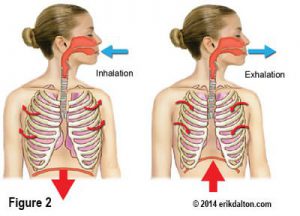
Although myoskeletal therapy delves deep into body structures, the intent is still slow and sustained soft-tissue work combined with specific client-initiated enhancers, such as chin-tucking, eye movements, deep breathing, pelvic tilting, etc. The client’s experience following a myoskeletal session should be one of invigoration, pain relief, increased range of motion and postural improvement. Bones are assessed and treated as soft tissues in the myoskeletal system, with pressure often applied directly to myofascia overlying transverse processes. It’s of the utmost IMPORTANCE to stress that bones only are used as levers to release hard-to-access, fourth-layer muscles, ligaments and fibrotic joint capsules (much like frozen shoulder work). Therapists always must remember that joints should never be taken into a nonphysiologic range of motion, which remains outside the scope of practice for most massage and bodywork practitioners.
On sale this week only!
Save 25% off the "Dalton Technique Treasures" eCourse

The “Dalton Technique Treasures” eLearning course is a compilation of some of Erik’s favorite Myoskeletal Alignment Techniques (MAT). Learn MAT techniques to assess and address specific sports injuries, structural misalignment, nervous system overload, and overuse conditions. ON SALE UNTIL April 29th! Get Lifetime Access: As in all our eLearning courses, you get easy access to the course online and there is no expiry date.