Engaging the brain, freeing the fascia
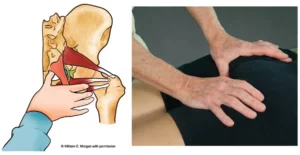
According to Cambridge Dictionary, the verb enhance means “to improve the quality, amount or strength of something.” Similarly, in Myoskeletal Alignment Techniques (MAT), the term enhancer is used as a noun to describe a therapist-directed movement cue that neurologically boosts, intensifies, and heightens a therapeutic outcome. In Image 1, I demonstrate and describe a MAT enhancer for a client presenting with excessive thoracic kyphosis and upper crossed syndrome.
Adding the enhancer to her MAT treatment boosted the involvement of her nervous system, allowing better rib-cage mobility, shoulder-girdle stability, and fascial front line extensibility. To help retrain her brain for this new posture, she was asked to perform the enhancer daily, preferably in front of a mirror.
MAT enhancers serve three primary purposes.
- Release musculofascial contractures
- Retrain the brain by introducing novel sensory information
- Reward the client through improved proprioception and body awareness
Case study: Treating whiplash with enhancers
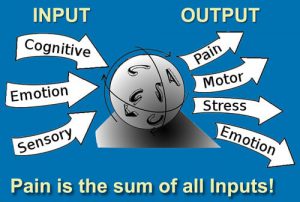
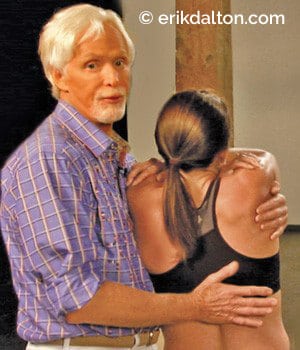
Ben was referred by an orthopedist for soft-tissue damage sustained in a rare side-to-side whiplash injury when his car was hit on the driver’s door six months earlier (Img. 2). The neck pain had subsided, but he could barely turn his head left and his orthopedist prohibited Ben from driving until he could turn his head to look in the rear view mirror.
Upon seated examination, his passive range into right cervical rotation, flexion, and extension was normal, but he could only manage 30 degrees of left rotation. A couple myoskeletal enhancers were used to determine if his primary restrictor was neural (protective guarding) or the result of residual soft-tissue damage. In many pain-free whiplash clients, the neck becomes sensitized and the brain will still perceive threat even though tissue damage to the area has long healed. In some cases, the use of novel movement enhancers can trick the brain into loosening the reins and dissolving the protective muscle guarding. Here’s a description of one of my favorite MAT enhancers that helped this client.

The seated treatment began by slowly rotating Ben’s head left to the first restrictive barrier and holding it there. His movement enhancer was to inhale deeply and slowly rotate his shoulders and torso as far right as comfortably possible several times and relax. Essentially, this maneuver is the same as asking him to turn his head left, but Ben’s brain did not perceive the torso-twist enhancer as threatening, and through graded exposure (pain-free repetition), his flexibility improved.
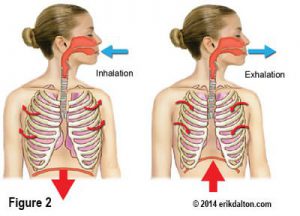
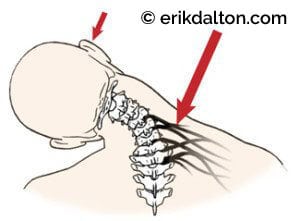
Then it was time to deal with the right-sided sternocleidomastoid (SCM) and upper-trapezius contractures that were visible as Ben turned to end-range. Image 3 demonstrates and explains a basic, but effective, MAT contracture routine that was chosen to conclude Ben’s first session.
Follow-up treatment
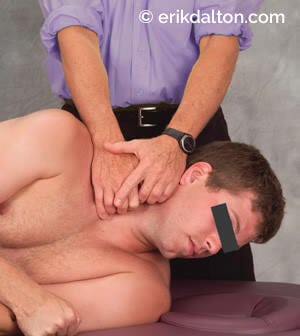
When Ben returned the following week, he was asked to demonstrate the torso-twist enhancer I’d ask him to practice daily in front of a mirror. I was impressed with his progress but still observed and palpated strain in his right SCM and at the base of his skull as he left rotated to end-range. Notice in Image 4 how my soft finger pads remain stationary, allowing Ben to left rotate at his tolerance level, and in Img. 5 how I use an optic-nerve enhancer via the suboccipital muscles to help align the atlas-axis joint.

During the three weeks of Ben’s treatment, I experimented with many myoskeletal techniques and enhancers, but those described in this article proved to be the most effective. Ben’s commitment to his MAT enhancer homework was a big plus in his recovery, which shortened his time with me and got him back behind the wheel.
References
- Postacchini F, Massobrio M, Idiopathic coccygodynia. Analysis of fifty-one operative cases and a radiographic study of the normal
coccyx. The Journal of Bone and Joint Surgery. 1983 65(8): 1116-1124. - Kim NH; Suk KS: Clinical and radiological differences between traumatic and idiopathic coccygodynia.
Yonsei Med J, 1999 Jun, 40:3, 215-20.
On sale this week only!
Save 25% off the "Dalton Technique Treasures" eCourse

The “Dalton Technique Treasures” eLearning course is a compilation of some of Erik’s favorite Myoskeletal Alignment Techniques (MAT). Learn MAT techniques to assess and address specific sports injuries, structural misalignment, nervous system overload, and overuse conditions. ON SALE UNTIL April 29th! Get Lifetime Access: As in all our eLearning courses, you get easy access to the course online and there is no expiry date.